Background
Wearable technology is quickly becoming the new normal in today’s healthcare environment. This emerging technology is driven by a combination of patient and physician preference. For patients, comfort, faster time to diagnosis and ease of use are at the forefront of the desire to use wearable devices. For physicians, the ability to gather data in a quick and efficient manner facilitates their ability to diagnose patients with minimal delays. One area quickly developing in the healthcare wearables industry is the wearable ECG patch. These devices are wire-free, lightweight, water resistant, single-use, disposable, and can gather quality ECG data. The case study below will describe how the wearable Cardea SOLO ECG Sensor was used in a Cardiology clinic setting to detect the early onset of Atrial Fibrillation (AF). Atrial Fibrillation is a public health concern as it is estimated that 2.7 to 6.1 million Americans’ are affected, and early detection is essential for limiting the risk of stroke associated with this condition.
Key Takeaways
- Cardea SOLO Sensor provided 99.4% analyzable ECG data
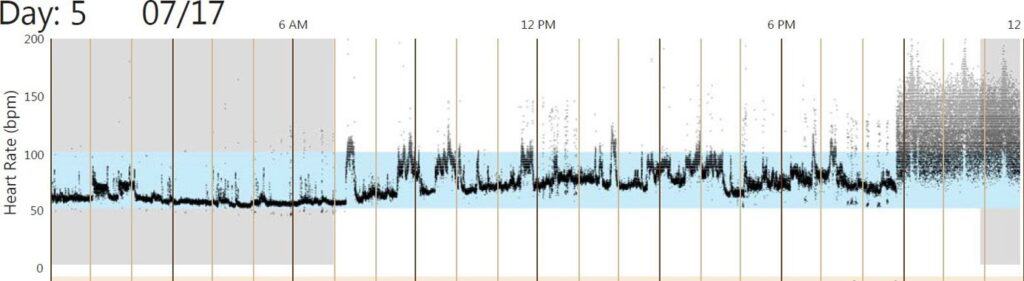
- Early onset AF detected on day 5
- Automated in-clinic software used in a Cardiology practice setting provides instant data needed to diagnose early onset AF