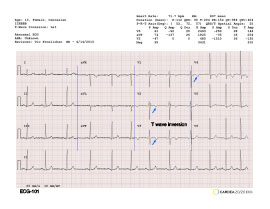
T wave inversion can be normal in female athletes in precordial leads V1 and V2 but it is abnormal when present in V4, V5 or V6. This ECG requires that an echocardiogram be performed prior to participation.
Click image to open extended view
ECG-102
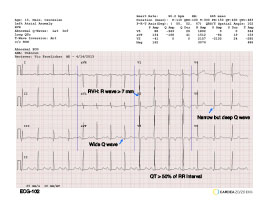
This ECG exhibits many of the criteria for HCM: Left Atrial Abnormality (LAA), Q waves and prolonged QT interval. The QT interval is usually prolonged if it persists thru more than half of the RR interval. This ECG requires that an echocardiogram be performed prior to participation.
Click image to open extended view
ECG-103
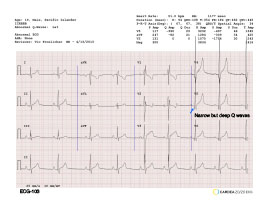
This ECG exhibits narrow but deep Q waves in the lateral leads consistent with HCM. This ECG requires that an echocardiogram be performed prior to participation. This can be a false positive and the probability of HCM is increased with each additional abnormality.
Click image to open extended view
ECG-104
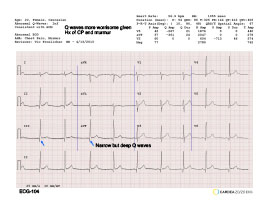
This ECG exhibits narrow but deep Q waves in the lateral and inferior leads consistent with HCM. This ECG requires that an echocardiogram be performed prior to participation. This can be a false positive and the probability of HCM is increased by the history of chest pain and a murmur.
Click image to open extended view
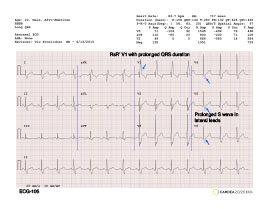
ECG-105
Per the features illustrated and the QRS duration of 140 msec, this ECG exhibits RBBB. It can be associated with congenital heart disease and pulmonary disease.
Click image to open extended view
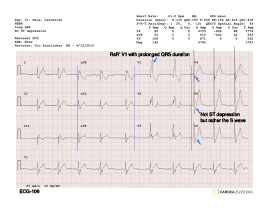
ECG-106
Per the features illustrated and the QRS duration of 150 msec, this ECG exhibits RBBB. It can be associated with congenital heart disease and pulmonary disease. Often the S wave can have a “shelf” that looks like ST depression.
Click image to open extended view
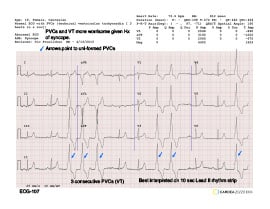
ECG-107
PVCs are rare in athletes but can be transitory and associated with allergies, alcohol, caffeine and drugs. This athlete exhibits technical ventricular tachycardia (3 PVCs in a row). The VT and history of syncope increase the risk of these findings. Referral for ECHO and evaluation by an electrophysiologist is appropriate.
Click image to open extended view
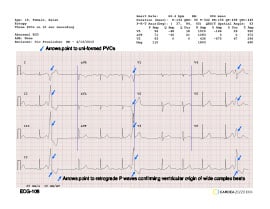
ECG-108
Three PVCs occurring on a 10-second tracing require further evaluation.
Click image to open extended view
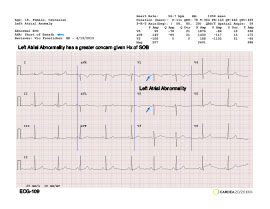
ECG-109
This ECG exhibits a Left Atrial Abnormality which can be due to hemodynamic alterations in the left atria due to mitral valve disease or ventricular stiffness (i.e., HCM). While not as worrisome when not associated with other ECG abnormalities it is more concerning in the athlete with dyspnea on exertion.
Click image to open extended view
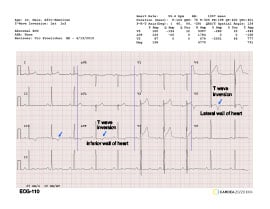
ECG-110
T wave inversion over the inferior and/or lateral surfaces of the heart can be due to hemodynamic or tissue abnormalities in the left ventricle and require an ECHO to be performed. In older athletes this could be due to coronary artery disease.
Click image to open extended view
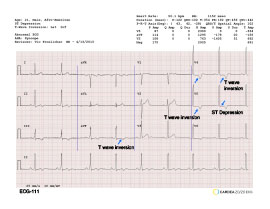
ECG-111
The T wave inversion and ST depression are suggestive of an LV cardiomyopathy (dilated or HCM) and an ECHO would be recommended. The reported syncope makes it even more worrisome.
Click image to open extended view
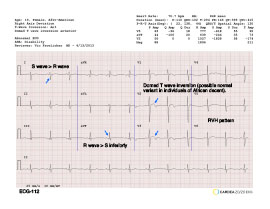
ECG-112
ST elevation with the appearance of a dome followed by T wave inversion in the anterior precordial leads can be a normal variant in athletes of African descent. It is apparently more common in Africans and less common in emigrants. This athlete also has right axis deviation and persistent S waves in V5-6 suggestive of right ventricular enlargement that can be a normal variant. These latter findings would trigger an ECHO prior to participation.
Click image to open extended view
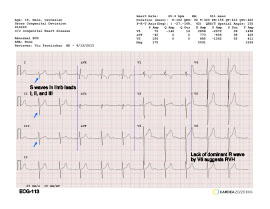
ECG-113
Right axis deviation and persistent S waves in V5-6 suggestive of right ventricular enlargement. The S waves in limb leads I, II and III (S123) are very suggestive of congenital heart disease and an ECHO should be obtained prior to participation.
Click image to open extended view
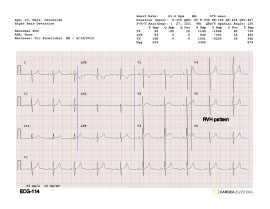
ECG-114
This athlete has right axis deviation and persistent S waves in V5-6 suggestive of right ventricular enlargement that can be a normal variant. These findings would trigger an ECHO prior to participation.
Click image to open extended view
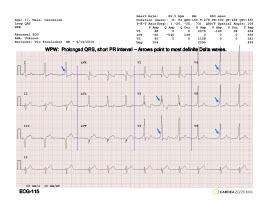
ECG-115
Classic WPW pattern with prolonged QRS, short PR interval and Delta wave of pre-excitation. This pattern mandates evaluation by electrophysiologist who can perform tests to see how fast the accessory pathway conducts. If it is too fast, dangerous arrhythmia can occur but these can be prevented by catheter ablation of the pathway.
Q waves or ST shifts are due to the abnormal activation of the LV and not other pathology. An ECHO is usually also recommended since WPW can be associated with cardiomyopathies.
Click image to open extended view
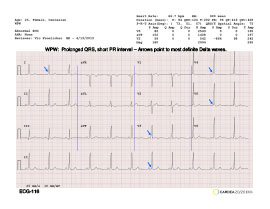
ECG-116
Classic WPW pattern with prolonged QRS, short PR interval and Delta wave of pre-excitation. This pattern mandates evaluation by electrophysiologist who can perform tests to see how fast the accessory pathway conducts. If it is too fast, dangerous arrhythmia can occur but these can be prevented by catheter ablation of the pathway.
Q waves or ST shifts are due to the abnormal activation of the LV and not other pathology. An ECHO is usually also recommended since WPW can be associated with cardiomyopathies.
Click image to open extended view
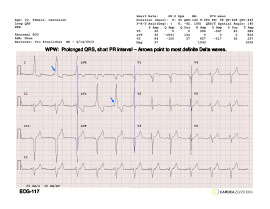
ECG-117
Classic WPW pattern with prolonged QRS, short PR interval and Delta wave of pre-excitation. This pattern mandates evaluation by electrophysiologist who can perform tests to see how fast the accessory pathway conducts. If it is too fast, dangerous arrhythmia can occur but these can be prevented by catheter ablation of the pathway.
Q waves or ST shifts are due to the abnormal activation of the LV and not other pathology. An ECHO is usually also recommended since WPW can be associated with cardiomyopathies.